Solutions to Alcohol and Other Drug Problems in Our Communities
Blueprint for a Comprehensive Treatment and Recovery System of Care - 2002
"An estimated 43% of the total population with AOD problems will be able to achieve successful recovery without formal treatment, utilizing Alcoholics Anonymous, Narcotics Anonymous, and other peer-based non-professional support programs."
Background
The
Community Recovery Network (CRN) - an organization of people in recovery
and family members and allies - spent four years developing and refining
a blueprint for a comprehensive treatment and recovery support infrastructure
at a level that is adequate to meet the needs of everyone with alcohol
and other drug problems (AOD) problems. We have also done extensive
research and held focus groups with a broad spectrum of people in the
treatment and recovery field in order to determine the cost of developing
and supporting the infrastructure.
Two
decades ago, the cost of going to treatment at a hospital-based program
was established at between $20 and $40 thousand dollars for a thirty-day
in-patient stay. Not only was this cost excessive, resulting in a severe
"back lash" of reduced AOD treatment benefits in the private
insurance industry, but there is no research evidence that thirty days
was an adequate treatment period. According to the National Institute
on Drug Abuse (1999), "Research indicates that for most patients,
the threshold of significant improvement is reached at about 3 months
in treatment. After this threshold is reached, additional treatment
can produce further progress toward recovery." Very successful
drug court programs retain clients for from one year to eighteen months,
and optimum program duration is sometimes even longer for adolescents,
people with co-occurring mental illness, and pregnant and parenting
women.
The
term infrastructure is important to our services proposal. In the past,
AOD services have been generally considered as programs. Ours is not
a plan to simply adding more programs to the current treatment system,
because the primary weaknesses we have identified in this system are
larger than the individual programs. These programs - while dramatically
under-funded for the work they do - tend to be isolated, fragmented,
and disconnected from each other and from the larger systems of public
health, social services, criminal justices, public safety, mental health,
and other institutions where AOD problems are most likely to surface,
such as families, schools, the workplace, and churches.
Our research, and the collective experience of CRN's constituency as expressed through surveys and focus groups, requires that any significant improvements in the current treatment system must include the following:
1. Services must be reimbursed that conform to research-based treatment principles and best practices. Treatment guidelines should include, at a minimum, those defined by the National Institute on Drug Abuse's "Principles of Drug Addiction Treatment" (NIDA, 1999) and by the Center for Substance Abuse Treatment's "TIPS," (CSAT, 2002), including especially, for adolescent treatment services, TIP 31: "Screening and Assessing Adolescents For Substance Use Disorders," and TIP 32: "Treatment of Adolescents With Substance Use Disorders," and the formal adolescent treatment guidelines developed by California's Department of Alcohol and Drug Programs (2002)
2. The treatment delivery system in each County must have intelligent mechanisms governing the authorization and utilization of services. Such management requires fundamentally that the decisions made about what services are appropriate to an individual client at what stage in his or her recovery and at what frequency need to be made by an entity other than the one that will provide the service and receive the reimbursement. These decisions also need to involve the client and family, and they must be made by an entity that is neutral to local political agency or "turf" issues to assure that utilization decisions are based to every extent possible upon what services will most likely result in the client's successful recovery.
3. Mechanisms need to be built into the system of care to enhance long term recovery as opposed to simply encouraging people to enter treatment. Some treatment administrators believe that the greatest current cost burden on the treatment system is not the individual who is a success and who therefore heavily utilizes services for a long period of time, but rather those who are failures - the individuals who access the system again and again but who never achieve recovery.
It is the belief of the CRN that the quality, consistency, appropriateness, and timeliness of services received should not be determined by any consideration other than that they are experiencing a problem with alcohol and other drugs.
Assumptions
For purposes
of illustration and of meeting Goal #2 of the Foundation for Addiction
Recovery, this Blueprint is applied to California; the same statistics
may be applied to any State. We have estimated the number of Californians
with AOD problems who are not yet in recovery at 2.5 million based on
the latest statistics published by the Substance Abuse and Mental Health
Services Administration (2002). In determining the investment required
for our proposed infrastructure to successfully serve all of these individuals,
we have made the following assumptions based upon research and surveys
of our constituency:
1. The involvement of family members in treatment and recovery support is essential to ultimate success. Based on our surveys, we are estimating an average of at 33 family sessions for each person served throughout the course of their treatment.
2. An estimated 43% of the total population with AOD problems will be able to achieve successful recovery without formal treatment, utilizing Alcoholics Anonymous, Narcotics Anonymous, and other peer-based non-professional support programs. The percentage is high because survey respondents were told that our plan includes comprehensive recovery-based case management services and family support for these individuals to assure that they find the programs that best meet their needs.
3. Of those remaining who require formal treatment, about 2/3rds will either be able to pay for treatment out-of-pocket or will be privately insured at a level that adequately covers the cost of treatment. According to the Substance Abuse and Mental Health Services Administration (1998), 70% or all the drug addicts in the U.S. and 80% of the alcoholics are in the workforce, and our advocacy plan includes achieving increased private insurance coverage for substance disorders.
4. The remaining 1/3rd will require publicly supported formal treatment services, either through California's Medi-Cal system or through direct subsidy supplemented by current state and federal Block Grant allocations. We estimate that the latter (about 75% of this State-supported group) will be able to make co-payments at an average of 20% of the total cost of their treatment. It is our belief that treatment should not be totally subsidized wherever possible, and that all programs should have sliding fee schedules for their clients based on income.
5. Paid public services are computed in five categories listed below. The first 2 categories are planned for the entire population. Not all of the people requiring formal treatment will need the last 3, but some may need more than one modality.
Category 1: Recovery-Based Case management services at $50 per hour with an average of 36 hours per client. This Case Management system will be privately contracted in each County and will also serve as the managed care mechanism for service authorization.
Category 2: Family counseling and support services at a rate of $100 per hour for an average of 33 hours for each client's family members.
Category 3: Inpatient medical detox / stabilization at a rate of $1000 weekly for an average treatment stay of 4 weeks. Our surveys indicate that 42% of those requiring public treatment will utilize this service.
Category 4: Outpatient Treatment, which includes outpatient detox using medications and acupuncture, and individual and group counseling and education. This is computed at an average cost of $5,000 for 52 weeks of phased treatment. Our surveys indicate that 58% of those requiring public treatment will utilize this service.
Category 5: Residential or inpatient services at a rate of $1000 weekly for an average client stay of 90 days. Our surveys indicate that 32% of those requiring public treatment will utilize this service. We draw a distinction between formal residential treatment and sober housing. The latter is non-licensed and organizations providing this service are generally self-supporting.
6. Accommodating the new treatment population will obviously have a significant impact on the existing system. To allow time to develop the capacity for new clients, we have projected that people requiring services would best enter the new system at the rate of 5% the first year, 10% the second, 15% the third, and 20% the fourth and fifth year, declining by the same rate through year 8, at which time all those in need will have entered the system. This entry rate will give the existing system an opportunity to "ramp up" the first four years to meet the new capacity needs and develop the infrastructure, and will also provide for a subsequent scaling down of services as service needs decline (See also the "Economic Impact" section below). Our projections assume an average success rate of 60% for the entire population in both the Case Management and Family Services Systems, and a 40% success rate for those entering the public treatment system. Research on various treatment populations and modalities show success rates ranging from 30% for the most severely impaired to 80% for those referred by Employee Assistance Programs and Drug Courts. Our projections therefore include a re-entry into the system each year of those unsuccessful the preceding years at these percentage rates. Like other chronic relapsing diseases such as asthma, hypertension, and diabetes, successful treatment for addiction requires often requires multiple treatment episodes before successful long-term recovery is achieved (McClellan, 2001).
7. We project California population growth of about 15% per year based on California Department of Finance estimates. We presume these new Californians will have AOD problems at the same percentage rate as the present population.
Systemic
Problems in the Existing Service System
Most modern treatment services for AOD problems have evolved in response to reimbursement mechanisms for the treatment of physical illnesses. While alcoholism and drug addiction have been identified by the medical and research communities as diseases, five very significant factors distinguish substance disorders from other diseases. These five factors must be systemically addressed in order to optimize successful outcomes in any system of care.
Distinguishing
Characteristics of Substance Disorders
1. Persons with other illnesses generally seek medical care when their condition becomes symptomatic. This is not true of persons with substance disorders due to the stigma, denial, hopelessness, impaired judgment, and other issues associated with AOD problems.
2. Persons with substance disorders typically have concomitant public health, mental health, and social issues whose resolution is tantamount to substance recovery.
3. While certain medical interventions for both acute and other chronic illnesses require behaviors or actions on the part of the patient in order for recovery or remission to be successful, long term recovery from substance disorders uniquely depends in most cases upon ongoing, patient-initiated activities and involvement with non-medical, non-professional, indigenous community resources (e.g. peer-support groups).
4. A Statistically significant number of addicted persons achieve successful recovery with these indigenous resources alone, requiring no formal treatment.
5. Some who are addicted achieve total remission with no outside help whatever ("maturing out" or "spontaneous remission,"), which is highly uncommon with any other chronic illnesses. This is most frequently found with persons addicted to nicotine and marijuana, and, less frequently, to heroin.
The most common indigenous community supports are the 12-Step Anonymous programs, but there are many other examples such as Women for Sobriety; Secular Organization for Sobriety; Rational Recovery; Native American Healing Circles; Religious, "Faith-Based," or other spiritual institutions, groups and societies such as the Calix Society, Jewish Alcoholics, Alcoholics Victorious, Alcoholics for Christ, and Mountain Movers.
Most of these are abstinence-based, but there are other "Harm reduction" indigenous support programs for persons on methadone maintenance, and there are also "moderate drinking" programs and a host of other alternative therapies for alcohol and other drug problems. It is important to note that there are stages and degrees of alcohol and other drug problems, and not all people with problems are alcoholics. Drinking and other drug problems are sometimes the result of life situations such as elderly persons who lose their life mate, or persons in combat or other traumatic settings.
The Absence of Effective Utilization Management in California's Drug-Medi-Cal System
The Sobky
v. Smoley lawsuit in 1994 ended limits on utilization of DM-C by ruling
that drug treatment is an entitlement under Medicaid guidelines. In response,
utilization of outpatient and day treatment services increased dramatically.
There were no caps on rates, and reimbursement occurred for clinic "visits"
only, not for specific services. While providers were required to have
perfunctory "Utilization Review Committees," ultimate decisions
concerning both utilization of services and the rates charged for those
services were being made by the service providers themselves without external
regulations.
Interestingly,
an analogous problem was occurring in the private sector; hospital-based
chemical dependency treatment programs were charging private insurance
companies thirty to forty thousand dollars and more for thirty-day residential
programs, often with no limitations on the number of patient repeat visits.
In short, the chemical dependency service delivery system - both public
and private - had become a fiscal "runaway train."
While the response
in the private insurance sector was either strict managed care practices
or the elimination of chemical dependency benefits altogether, the response
of the DM-C system in 1996 was cost containment achieved by constricted
services such as limits imposed on rates and on the number and kinds of
services a client could access. The DM-C system appeared - because of
Sobky v. Smoley - unable to adopt the kinds of managed care strategies
that characterized other venues. The services received by clients under
DM-C, therefore, came not to be based on clinical guidelines or recovery
principles but rather on constrictions devised to contain costs. These
constrictions remain in place today.
Not only are
such constrictions without reference to our knowledge about successful
recovery, or to research-based clinical principles or science-based treatment
practices, but they sometimes frustrate the goals of other State-sponsored
services and result in far greater costs than those that were "saved."
For example, a chemically dependent pregnant woman on the caseload of
Child Protective Services will be eligible for DM-C services during her
pregnancy, but her eligibility will be removed shortly after her child
is born. With non-DM-C perinatal day treatment services experiencing dramatic
waiting lists in many Counties, this can result in substance relapse,
loss of custody of the child, and the ultimate failure of family reunification.
Or a chemically dependent severely mentally ill person who is in need
of comprehensive residential treatment will find that it is not a covered
Medi-Cal benefit and hence unavailable in the County, resulting in psychiatric
emergency. In these cases, the "cost containment" measures result
in costs to the State that are far greater than those of treatment, such
as out-of-home foster care placement and exorbitant psychiatric emergency
services.
Not surprisingly,
these "cost containment" measures in 1996 were soon followed
by the elimination of State mandates for providers to perform the monthly
utilization review that had provided the only mechanism of outside monitoring
of quality assurance in the system. Although an annual Utilization Review
mechanism was to have been instituted by the State, this has occurred
only sporadically, and the only specific control on provider utilization
of DM-C is the occasional and expensive provider audit.
Recovery-Based
Case Management
Both the five
distinctions of substance disorders listed above, and the absence of utilization
management in California and many other jurisdictions, suggest a critical
need for comprehensive and diverse case management services. But the recovery
community's collective experience suggests that traditional case management
as utilized in the health and mental health systems of care may not adequately
or appropriately address all of these unique characteristics of substance
disorders.
Our blueprint therefore recommends a "Recovery-Based Case Management" System in each local jurisdiction. The system would be operated under contract with the State or County by a private entity who was not a treatment service provider (click here for "Guidelines for an Entry Level Recovery Advocacy and Case Management System).
Recovery Advocacy
in the AOD treatment system is not an unprecedented concept. Many drug
court venues in California and around the country have adopted a "Court
Liaison" function - a person who mediates between the court, probation,
and treatment system on behalf of the client or offender. The role of
the Liaison is to assess and explain options to the client, to propose
referral recommendations to the drug court judge, and then to "leave
no stone unturned" in assuring that the client is successfully engaged
and retained in the recommended services. Many Counties in California
adopted a similar "recovery advocacy" model for their perinatal
case management services, and similar case management services were successfully
provided to SSI recipients before the elimination of the alcoholism and
drug addiction disability benefit.
The recovery
community has learned that not everyone with AOD problems needs formal
treatment. For many people, 12-Step and faith-based activities and their
equivalent, which may or may not be in combination with clean and sober
housing, are adequate for successful recovery. The proposed system would
be distinguished from traditional case management services that are used
in the public and private health sector in that their primary objective
would not be exclusively clinical (e.g. to access clinical services),
but to assist the client in engaging in those natural community supports
that enable long term recovery.
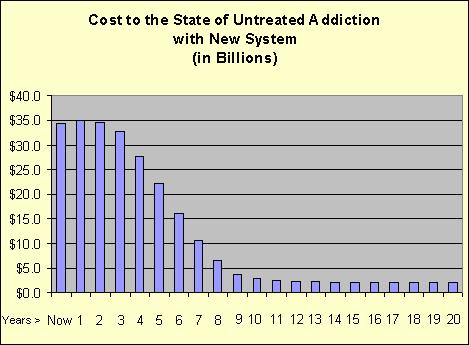
The
Return
The State will experience a significant return on this investment. The ultimate return is illustrated in the chart below. The chart begins on the left with the current cost to California State government of untreated AOD problems - $34 Billion. The increase over the first three years results from the cost of the new treatment investment. During the initial few years, this return is a theoretical one only. The reason is that the State government is now heavily invested in a massive infrastructure (14.3% of its 2002 budget) to address untreated AOD problems, and it will take some time to begin to downsize these bureaucracies of public health, criminal justice, social services, mental health, and public safety.
Because
it is always the natural tendency of government to expand, a significant
continuing role of the Foundation will be to monitor the decline of these
wasteful services and to advocate for their appropriate reduction. There
will be an eventual commensurate decline for Californians in the costs
of such things as automobile and health insurance, and in goods and services,
whose current prices reflect the significant loss in productivity that
results from untreated AOD problems in the workplace.
It
is interesting to note that part of the reason that AOD problems have
not been addressed in the past is that the benefits do not accrue within
the tenure of any of our elected State offices.
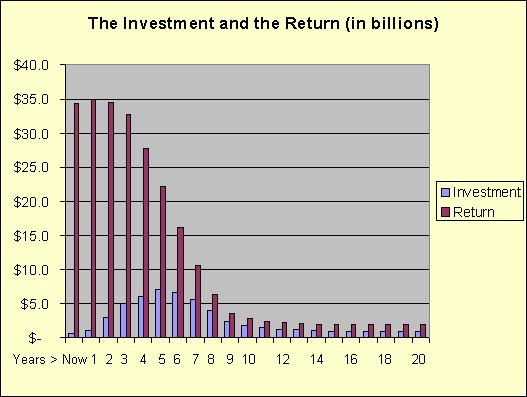
For purposes of comparison, the chart below shows both the projected treatment investment and the return. The red (dark) bars and the blue (light) bars represent respectively the cost of untreated AOD problems and the proposed treatment investment. The ones furthest left represent the current relationship of a $34 Billion cost and a $600,000 investment. Note again that the cost is always higher than the return because it is a combination of the investment plus the cost of remaining untreated AOD problems.
Citations
CASA
(2001), "Shoveling Up: The Impact of Substance Abuse on State Budgets."
The National Center on Addiction and Substance Abuse at Columbia University.
McLellan,
Thomas; Lewis, David; O'Brien, Charles, and Kleber, Herbert (2000). Drug
Dependence, a Chronic Medical Illness: Implications for Treatment, Insurance,
and Outcomes Evaluation. Journal of the American Medical Association.
284:1689-1695.
NIDA
(1999). Principles of drug Addiction Treatment: A Research-Based Guide.
National Institutes of Health, U.S. Department of Health and Human Services.
NIDA/NIAAA
(1995). The Economic Costs of Alcohol and Drug Abuse in the United States-1992,
Executive Summary. National Institute on Drug Abuse/National Institute
on Alcohol Abuse and Alcoholism, 1995.
Substance
Abuse and Mental Health Services Administration (1998), "National
Household Survey on Drug Abuse," U.S. Department of Health and Human
Services. Rockville, MD.
Substance Abuse and Mental Health Services Administration (2002), "National Household Survey on Drug Abuse," U.S. Department of Health and Human Services. Rockville, MD.
White House Office of National Drug Control Policy (2001), The Economic Costs of Drug Abuse in the United States 1992 - 1998.
Why Add Acupuncture to your Treatment Program? FAQs